
I see a lot of patients with hip pain. Many times, the pain comes on slowly and insidiously out of nowhere without a specific incident which the patient can blame for its onset. Sometimes they recall a fall after which the outer aspect of the hip persists in being sore to touch, at times with walking, and worse yet when trying to sleep at night. In such circumstances, hip bursitis is often the underlying cause.
The hip abductors are a group of muscles on either side of the body that connect the pelvis to the thigh bone and support us when we walk and position the legs away from the midline of the body. This action is called hip abduction and relies on the healthy function of two main hip abductor muscles, the gluteus medius and gluteus minimus. Around these muscles and the portion of the thigh bone on which they insert is a tight fascial structure that runs from muscles coming off the pelvis all the way to the knee called the iliotibial band (ITB).
Between this ITB and the prominence of the upper part of the thigh bone at the hip joint is naturally a bursa which acts to create a frictionless interplay between this thigh bone prominence and the ITB. When this bursa is inflamed whether from trauma or tightness of the overlying ITB, this is what we call hip bursitis, specifically trochanteric bursitis.
Trochanteric bursitis affects adults of all ages. You can feel your own trochanter as the bony prominence along the lateral border of the upper thigh at the hip. Luckily, bursitis of the hip often responds to conservative treatment that may involve strengthening the muscles around the hip as well as a stretching program for the ITB. A steroid injection given at the bursa also can help for a lengthy period of time. When lateral hip pain persists despite such treatment, that’s when it makes sense to consider surgical intervention.
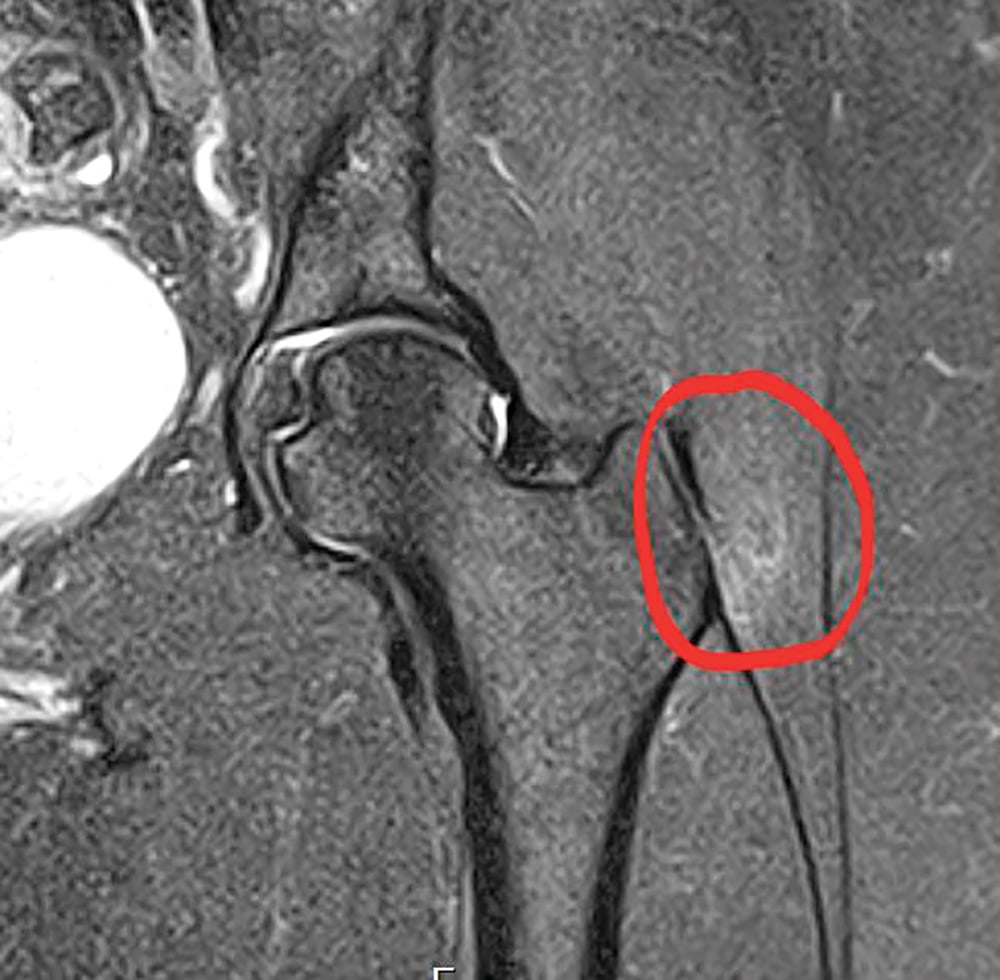
Recently we treated such a patient, a 46-year-old woman whose hip was injured after falling on her left side. She had done physical therapy for two years and had responded only for a limited time after trying steroid injection therapy. The circled area of the MRI shows the area of inflammation and bursitis. The ITB is the vertically oriented black linear structure seen just lateral to the inflamed bursal region.
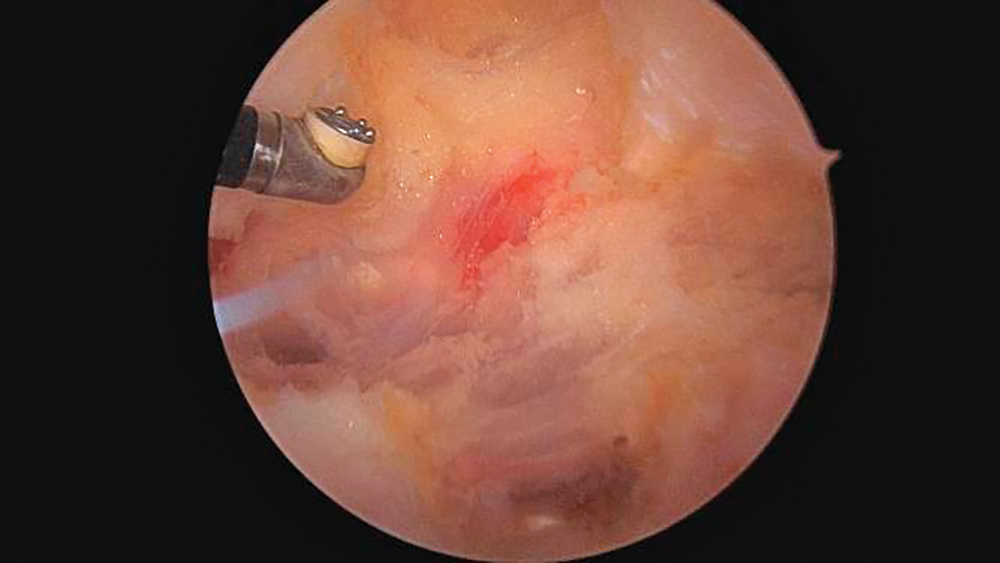
So this patient opted for surgical intervention, which involves releasing the ITB to decompress the pressure placed by this fascial structure over the trochanteric bursa and also involves removing the inflamed bursa itself. This is accomplished by making two tiny incisions about one centimeter long each and with a camera through one incision and a radiofrequency device through the other, we can perform the release. The photos show what the ITB looks like before and after the release.

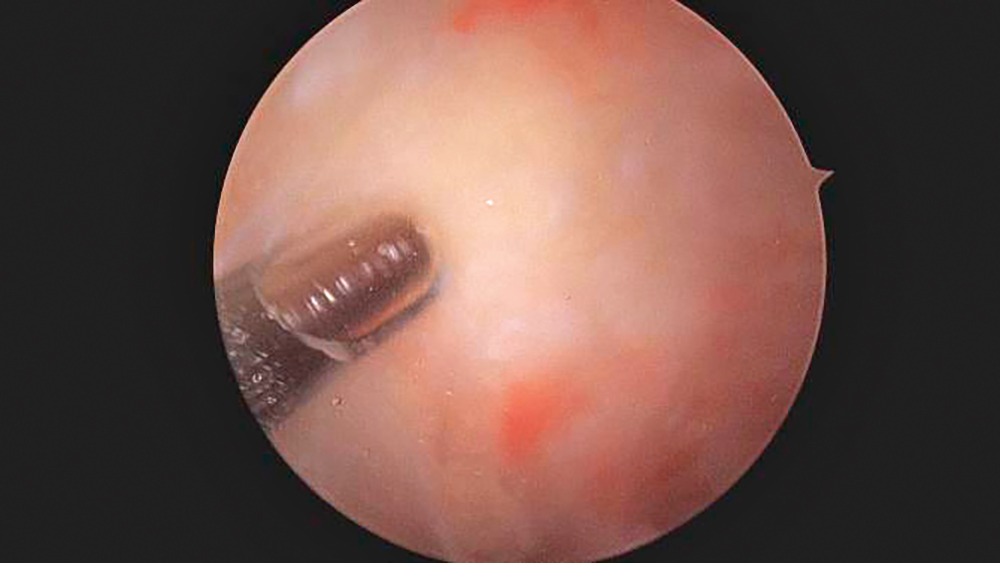
We use this opportunity to also evaluate the underlying tendon insertions of the gluteal muscles on the trochanter to make sure there are no tears that could also be causing pain. Her trochanteric tendons looked healthy and intact as seen here.
After this 20-minute procedure, patients are immediately allowed to walk without restrictions and this patient in particular has gone on to do quite well with her pain resolved. If you are experiencing such chronic pain along the lateral aspect of your hip, please don’t hesitate to come in for a thorough evaluation!
Dr. Heitman is an orthopedic surgeon at The Center for Musculoskeletal Disorders specializing in all kinds of sports injuries related to knee, hip, elbow and shoulder.






