
“Empowering function through education” series.
“I have pain in my shoulder. Is it my rotator cuff? Where is my cuff? Someone told me I have bursitis. Do I have bursitis? What’s a bursa?”
Shoulder impingement is one of the most common causes of shoulder pain in adults. People with this condition typically experience pain in the front or the side of their shoulder, particularly with overhead activities, resulting from bursitis and/or tendinitis of the rotator cuff tendon. Shoulder impingement occurs when the top outer edge of your shoulder blade, called the acromion, rubs against (“impinges on”) or pinches your rotator cuff tendon or the bursa (a sack of fluid that cushions the tendon) beneath it, causing pain and irritation. We see many patients with this diagnosis in our practice, and many of their questions are similar. Since it is so common, we figured we’d tackle this topic next. So what exactly is shoulder impingement and what causes it? First we need to understand the anatomy of the shoulder to understand what is happening.
Anatomy Lesson (Don’t Worry, We Won’t Make It Too Boring)
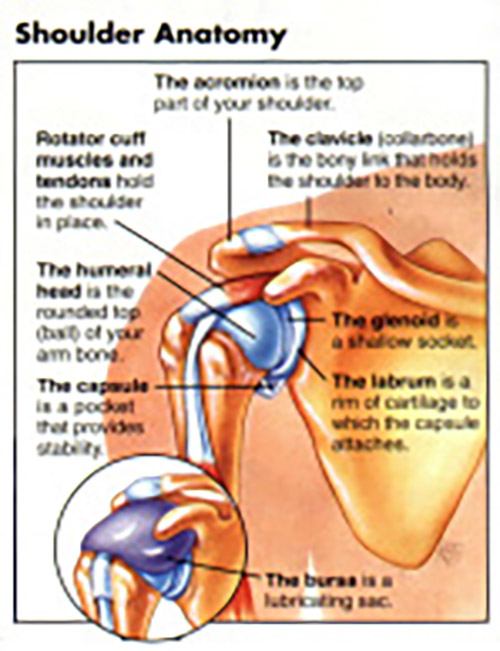
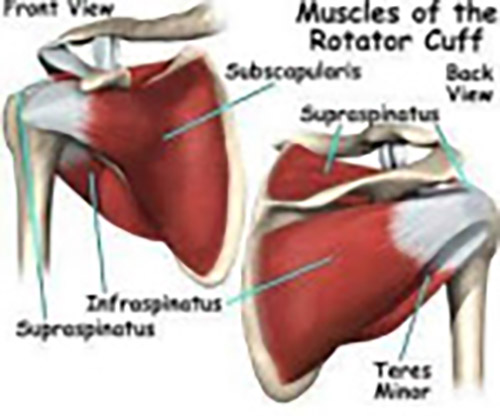
The shoulder complex is actually comprised of several connecting joints, tendons and muscles. Today we will focus on the Glenohumeral (GH) and Acromioclavicular (AC) joints, as well as the rotator cuff and the bursa. The GH joint is a ‘ball-and-socket’ joint. A “ball” at the top of the humerus (upper arm bone), fits neatly into a “socket,” the glenoid, which is part of the scapula (shoulder blade). The shoulder blade has a hook at the top called the acromion. The acromion hooks over the top of the shoulder and connects with your collarbone, called the clavicle, creating the AC joint. The scapula rests on your upper back and is the foundation for the movement of your shoulder. In order for you to raise your arm, the shoulder blade has to turn/rotate out and up, to give your humerus room to turn and lift so that you can reach overhead. Now a quick spotlight on the famous rotator cuff. The rotator cuff is essentially a name given to a collective four muscles: The supraspinatus, infraspinatus, subscapular and teres minor muscles. These muscles have two functions. The first is to rotate the shoulder joint: three rotate your shoulder outward (external rotation) and one rotates your shoulder inward (internal rotation). The second, more important, job is to stabilize the joint while you move. When you hold your arms out like an airplane, your rotator cuff is working very hard to keep everything where it should be.
One of your rotator cuff muscles, the supraspinatus, passes under the tunnel created by your AC joint to insert onto the head of your humerus. Above the supraspinatus tendon, sits a bursa, or a sack of fluid, to cushion the tendon against the AC joint.
This, my friends, is where all of the magic, or in this case, the mischief, happens. Inflammation under your AC joint caused by irritation of the bursa or the tendon, or both, is the most common cause of impingement. As a result of the inflammation in that small tiny space, every time you try to lift your arm, the tendon and bursa get squished by the diminished space created by inflammation, and you remain with a shoulder that hurts every time you reach overhead.
Causes of Impingement
So what causes impingement (or the inflammation under your AC joint)? “Overuse is the leading cause of shoulder impingement.” You’ll see this statement everywhere, and it is true; however, it’s not the full story. If your job requires you to reach overhead all day everyday, yes, that repeated movement will likely cause impingement. Impingement pain may also develop as a result of a minor injury in which there is impact, such as a fall onto the shoulder or outstretched hand. However, poor posture, scapular and shoulder weakness, and poor scapular biomechanics resulting from weakness is usually at the root of the problem.
Let’s talk about weakness first. Your rotator cuff is supported by all of your scapular muscles, particularly those that pull your scapulas together (retraction) and move them apart (scaption). These scapular muscles help to anchor your scapula (or shoulder blade) to your back and help to turn, or rotate, the shoulder blade, in order for you to lift your arm overhead. If these muscles are weak, they can’t anchor your shoulder blade nor can they rotate it well, and so your rotator cuff is left with more work. Your cuff isn’t made to take on that additional work, and so that will result in fatigue and ultimately inflammation at the tendon, aka tendonitis. Additionally, if the shoulder blade muscles can’t rotate your shoulder blade to clear your upper arm for movement, the head of your humerus will push your cuff tendon and bursa into the ac joint everytime you lift your arm, impinging on the tendon and bursa. Now let’s talk about posture. Posture doesn’t have to be “very poor” to create problems. Any degree of forward shoulders, mild to severe, can cause the issue. If it’s mild, it might take longer to develop, whereas moderate to severe can cause ongoing pain.
Forward shoulders place your shoulder blades further away from your spine. As a result, the shoulder blade can’t rotate as it needs to in order to allow your arm to clear the overhead reach. What ends up happening is that because the shoulder blade can’t turn, your humerus pushes the tendon and bursa into the AC joint, aggravating them and creating inflammation every time you try to lift your arm overhead. This creates a repetitive motion injury. I know what all you people with shoulder pain are thinking. If only you listened to your mothers when she said, “Stand up straight.” It is important to note that shoulder separation, shoulder dislocation and the infamous Frozen Shoulder also place you at risk for impingement.
Frozen Shoulder is a beast unto itself and we will try to address that in a future article. If you are physically unable to lift your arm past 90 degrees, where your shoulder is not just painful, but it’s physically stuck, please go see a doctor asap. A physiatrist or orthopedist is the way to go.
How Do I Know If I Have Shoulder Impingement?
Regardless of the cause, impingement can lead to a number of symptoms in your arm. Common symptoms include slowly developing shoulder pain that comes on for weeks or months, pain along the front or side of the shoulder that may travel down the side of the upper arm, pain when moving your arm to the side or overhead (very common to have hand pain with reaching for your seatbelt), pain that interrupts your sleep or prevents you from lying on the affected side, difficulty reaching behind your back (like reaching for your back pocket), and shoulder stiffness or weakness. If you are experiencing these symptoms, the first thing to do is consult with your doctor. Your doctor may order some tests such as an MRI, or may send you straight to physical therapy. In New Jersey, patients have direct access. That means that if you want to start with physical therapy (some patients prefer this due to time constraints or personal success stories with previous rounds of PT), you are legally allowed to do so without an MD referral for 30 days. However, after 30 days, you will need a prescription. We can also help to guide you on what kind of doctor to see.
Now to the Good Stuff … Treatment
Can We Make Your Shoulder Pain Go Away? Yes!
Conservative treatment for shoulder impingement includes rest, nonsteroidal anti-inflammatory drugs (NSAIDs) such as Advil or Aleve (please speak to your doctor first), ice to decrease the inflammation, and, of course, physical therapy. In a study by Wesley et al, in 2013, they demonstrated that 10 weeks of physical therapy both improved function and reduced pain in people with shoulder impingement. The duration of healing will vary, however, depending on the individual case. In cases where the body does not respond to these conservative treatments, doctors may recommend an injection, as well as more testing. When all else fails, doctors may recommend surgery (argh). All that being said, shoulder impingement usually responds very well to physical therapy, which uses manual techniques and various exercises, as well as techniques to re-educate the shoulder complex, in order to improve symptoms.
The first step is a physical therapy evaluation, which is used to “put the pieces together”and solve the root cause of your shoulder pain. As with all injuries, it’s important to start with a good history. How long ago did the pain start? What were you doing when you first felt it? Has it worsened? Has it spread? What do you do for a living? For recreation? A good history helps us determine the cause of injury and also helps us identify risk factors that may be predisposing you to injury. For the physical part of the evaluation, we will use special tests and measures to assess the biomechanics of your shoulder and where it’s going wrong. PTs use special tests, in addition to observing your posture, observing how your shoulder blade moves compared to your arm, measuring range of motion (ROM) and strength, and may even evaluate your neck (sometimes shoulder pain can come from the neck, stay tuned for a future article on cervical radiculopathy). Your physical therapy sessions will likely focus on the biomechanics of your shoulder complex and the muscles in your shoulder, arm and chest. Ultimately, we want to improve the function of your shoulder blade and rotator cuff, as well as re-education of the shoulder complex as a whole. If you’re an athlete or work in a field that requires frequent use of your shoulder, we can teach you proper techniques and ergonomics to reduce your chance of recurrence. We may also give you some exercises that you can do at home, which can help you recover faster (Just make sure you don’t overdo it).
Typically physical therapy begins light with basic ROM exercises with the goal to decrease pain and inflammation. Treatment will consist of a lot of manual therapy and gentle exercises. Once you achieve full and mostly pain free ROM we will start progressive strengthening.
Strengthening the muscles is crucial and research shows that this gives you the best long-term outcome! As you start to get stronger and maintain your mobility, your pain will continue to decrease if it is not already gone. Your increased strength will allow you to perform more activities and prevent flare-ups. This usually does take up to four to six weeks. Once you are mostly recovered, we can start easing you back into sports and recreation, like golf, tennis, exercise or whatever your favorite activities are. This is when we start winding down treatments and getting you back into functional strengthening, sport specific training, and whatever your goals are. In the end, we reassess everything, making sure we achieved all of your goals, that all risk factors are gone, and finalize your long-term home exercise program. Most importantly, throughout the entire process, we will be providing you with lots of our favorite topic, patient education. This includes educating you about your condition, making recommendations for posture, the amount of exercises you perform, your home or work activities, and your athletic activities.
Lastly, it’s important to remember that we see this diagnosis often, but each person is different, with different biomechanics and different stresses. When treating someone with any diagnosis, it’s important to treat the person, not the injury. Physical Therapy is so much more successful when we treat you, educate you, help you understand what’s happening, listen to your goals, and include you and your specific needs in the plan of care. No matter where you go, make sure the therapist listens to your needs. Are you looking to get back to exercising? Return to playing ball with your son or grandson? Return to performing a specific exercise like pull ups? At Prime Orthopedic Rehabilitation, we reserve an hour to sit with you one on one, to ensure that we can offer you the best chance at success.
Here at Prime, we’ve got your back … and your shoulder;).
Prime Orthopedic Rehabilitation
111 Dean Dr,
Tenafly, NJ 07670
(201) 503-7173
www.Prime-Rehab.com
To make an appointment, please call the office.









