What do the Dominican Republic and the island of Kyushu in Japan have in common? Read on.
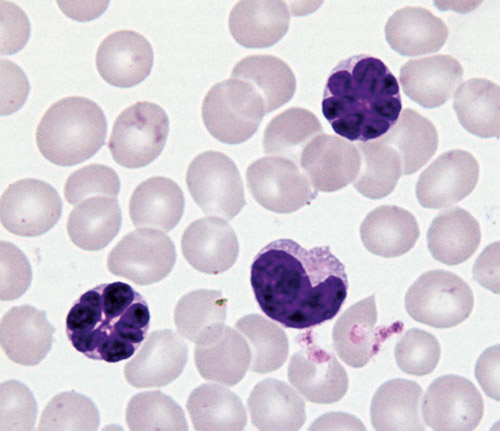
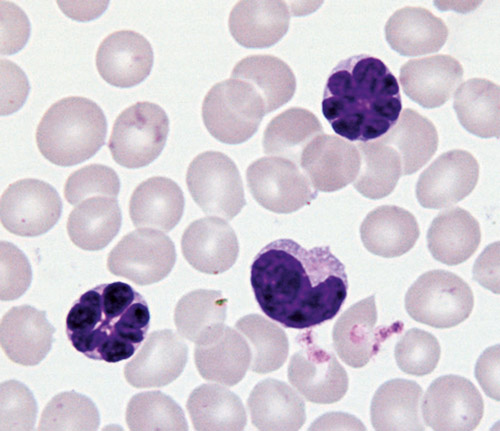
Adult T-cell leukemia/lymphoma (ATLL) is a type of non-Hodgkin lymphoma which is very uncommon. Lymphomas have as their cell of origin a type of white blood cell called a lymphocyte, a cell which is part of the immune system. There are two types of lymphocyte—B cells and T cells. The majority of lymphocytic malignancies (leukemias or lymphomas) arise from B cells—T cell-derived malignancies are less common and tend to be more aggressive and difficult to treat.
ATLL is a particularly virulent type of malignancy with a high mortality rate, so it is fortunate that it is rare. Its incidence rate in the U.S. is 0.05/100,000 annually—thus, there are probably only about 100-200 cases annually in the U.S. The disease is characterized by fatigue, enlarged lymph nodes, an enlarged spleen, rash, and hypercalcemia.
But there are many rare tumors and I have been selecting tumors to discuss that have something interesting to teach us. There are populations in which the incidence rate of ATLL is dramatically higher. Specifically, it was noted that it clustered on the southern and northern islands of Japan, primarily Kyushu (the island on which Nagasaki is located) and in the Dominican Republic. Indeed, the disease itself was first identified as a distinct entity in 1977 by Japanese pathologists. In the high incidence areas, its incidence rate is as high as 27/100,000 annually—there are 700 cases each year in Japan. And because there has been a large influx of Dominican migrants to New York City, centered in northern Manhattan and Washington Heights, there is also a blip of ATLL in that community as well, so my own hospital which is located there sees an unusual number of these cases.
But what is responsible for this tumor and what explains its geographic distribution? To answer this, we need to go back to 1981 with the beginning of the AIDS (acquired immunodeficiency syndrome) epidemic. AIDS is also a T-cell disorder, albeit not a malignancy, that results in a weakened immune system. Scientists quickly focused their attention on identifying its causal agent, presumably a virus, and HIV (human immunodeficiency virus) was isolated and identified in 1983 at the Pasteur Institute in Paris.
Skip ahead to the 2008 Nobel Prize in Medicine, one of the more controversial awards in recent times, which was awarded to Luc Montagnier and Francoise Barre-Sinoussi, the two French scientists who accomplished this feat. (A third winner who shared the award was Harold zur Hausen for discovery of human papillomavirus and its association with cervical cancer.) Why was this prize controversial? Because missing from this award was Robert Gallo of the National Cancer Institute whose paper isolating HIV was published in 1984, one year later. However, he developed previously (before 1981) the techniques and methods utilized for identification of the virus by both groups, i.e., by the French as well as his own group.
What is important to us with regard to ATLL is that when Gallo (who I think was robbed) published his isolation and identification of HIV, he called it HTLV-3, Human T-cell Lymphotropic Virus 3. This was a revolutionary new type of virus, a so-called retrovirus. When we were taught molecular biology in my day, we were taught that DNA is transcribed to make RNA, and that RNA is translated to make protein and that DNA replicates itself. Thus, all of the known human tumor viruses at the time were DNA-containing viruses so that the virus could insert DNA into the healthy cell’s genome and thereby induce malignancy.
But Gallo (and others in animal and avian studies) had discovered that there are RNA-containing viruses that contain an enzyme, reverse transcriptase, which can go backwards, in reverse, and transcribe RNA into DNA so that it can be inserted into the cell’s DNA genome. This was a revolutionary new concept; the first viruses in humans identified as being RNA-containing retroviruses of this type were the HTLV viruses. The fact that HIV was HTLV-3 implied that there was a previous HTLV-1 and HTLV-2 virus. And who was responsible for isolating and identifying HTLV-1, the first human retrovirus? Robert Gallo. What was later done by the French for HIV was simply replicating his techniques.
So what and when was HTLV-1? This was published in Nature by Bernard Poiesz working in Gallo’s lab in 1981—they clearly established that infection with HTLV-1 was responsible for the clusters of cases of ATLL in Japan and the Caribbean. It is believed that the high rate of infection in Japan is due to maternal-fetal transmission while the high rate of transmission in the Dominican Republic is thought to occur through sexual transmission. HTLV-1 also appears to be transmitted by needle sticks among drug users and so the prevalence rate of HTLV-1 among IV drug abusers in the U.S. is very high. Luckily it does take decades following infection for the disease to appear.
Alfred I. Neugut, MD, PhD, is a medical oncologist and cancer epidemiologist at Columbia University Irving Medical Center/New York Presbyterian and Mailman School of Public Health in New York.
This article is for educational purposes only and is not intended to be a substitute for professional medical advice, diagnosis, or treatment, and does not constitute medical or other professional advice. Always seek the advice of your qualified health provider with any questions you may have regarding a medical condition or treatment.









