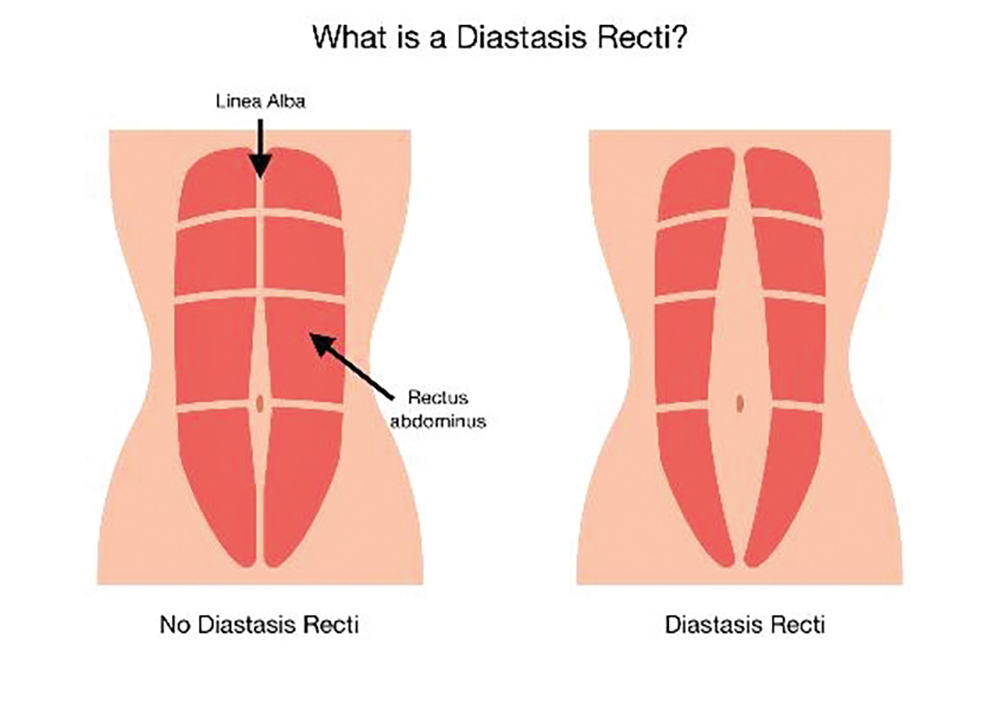
What is Diastasis Recti (DR)?
During pregnancy, there is a widening of the space between the two sides of the abdominal muscle called the rectus abdominis in order to allow for stretching of the belly for a growing baby. This happens during every pregnancy and is completely normal. Usually, within about 8-12 weeks postpartum the abdomen goes back to its regular resting place without a gap between the sides. However, in some women the rectus abdominis remains stretched for longer, and a space remains between the two sides, as well as a slacking of the tissue beneath the center, allowing for “doming” or what many women will describe as “still looking six months pregnant.”
Why do some women get persistent DR and some don’t? Is it due to my baby’s size?
The honest answer among all the current research on DR is that nobody knows definitively why some women have DR for an extended period of time and some women’s abdomens “bounce right back.” In my experience as someone who has treated many postpartum women both with and without DR, I can say that I have seen women who have had twins and never exercised during pregnancy and do not have DR postpartum, and I have seen women who took prenatal pilates all nine months of pregnancy and had a 6-pound baby and have significant DRs postpartum. The bottom line is: Each body is different.
Is having DR dangerous? Will it cause back problems? Do I need to fix it if I have one?
Like most answers in the medical sciences field, it depends. As physical therapists, we are looking mainly for the level of functional deficit any diagnosis is causing. We know that the stretching out of the abdominal wall which causes DR often is associated with weakness in the abdominal muscles or the “core.” When the core is weak there can be an increased strain on the back muscles as compensation to hold the body upright or to lift something heavy, which over time can lead to back pain. However, not all DRs look and behave the same. Some women with a technical DR, meaning they have separation of their rectus abdominis, have strong core muscle underneath the top layer of tissue and are fully functional and without pain. So, the answer to the question if you need to treat every DR would be: “Does it bother you?” If there is pain or weakness or other symptoms associated with it (possibly pelvic floor related symptoms), or if the aesthetics of the doming abdomen is bothersome to you, then yes you should seek treatment. Otherwise, keep doing what you’re doing to stay strong and active.
What are my treatment options for DR? How long does it take to “fix,” and will I have a flat stomach after treatment?
I will readily admit my bias as a physical therapist and have more expertise in that field than others, but typically there are two options if you decide to treat the DR: 1) physical therapy. 2) plastic surgery.
I tell all my DR patients that tissue in the body takes a long time to change. When being treated for DR conservatively, the patient should expect to see the maximal results within about 1-1.5 years. My goal as a physical therapist is to get the patient as strong, functional and independent as possible; then the patient usually continues with the exercises and tips on their own for the rest of the rehabilitation time. Pregnancy causes many physical changes, including rib cage positioning, breathing pattern changes, pelvic floor weakening and posture changes that can all contribute to a non-healing DR. Therefore, treatment of the DR should always include evaluating and treating each of these areas in addition to the strength of the core muscles to help set the body up for the most successful healing process. It really is a whole-body approach.
With that being said, I never promise a flat stomach by the end of the treatment. Some of the most severe DRs will not fully come back together even with the best training and treatment. Additionally, sometimes we can get the patient strong and functional, but the elasticity of the skin and muscle stays very loose and the bulge remains even without the weakness. In such scenarios the only true option for the flatter abdomen is plastic surgery. I will say that even if you opt for plastic surgery from the beginning, muscle weakness cannot be fixed with surgery. This person will still need guided strength training post-surgery to have a strong and functional body.
How do I know if I have DR?
You can test yourself by lying flat on the floor and placing two fingers perpendicular to the line between your belly button and your pelvis (and then also above the belly button). Then lift your head and shoulders off the floor like you are doing a mini crunch. If you feel your fingers sinking down with the abdominal muscles forming to the sides of your fingers, you may have DR. If you feel firmness beneath your fingers, you are probably good! If you are not sure, you can set up an evaluation with any physical therapist in the area who treats women’s health issues.
Should I avoid certain exercises like planks and crunches if I have DR?
Research is always changing and evolving. The PT world, as recently as about 10 years ago, suggested avoiding putting excess pressure on the front of the abdomen with exercises such as crunches and planks, with the thought that they may worsen the DR or not allow it to heal. However, all of the current literature on the topic, as well as diagnostic ultrasound, has proven that this is not entirely correct. In fact, in order for the muscle and tissues to get stronger and firmer, we need to load them progressively, the same way we do strength exercises on leg muscles after a knee injury. However, I would suggest at least having some guidance from a trained professional in this area to pinpoint all the muscle groups that need to be targeted and how to safely progress the exercises or address any other issues that may be preventing healing.
Deena Elias is a physical therapist from Teaneck. She graduated from Hunter College in 2011 with a doctorate in physical therapy. She has a background in outpatient adult orthopedic physical therapy. Deena is the owner of Personal Physical Therapy, which provides private physical therapy to people in their homes and specializes in women’s health, including pregnancy, postpartum care, and pelvic floor training. She can be reached by email with any questions or comments at [email protected].






