
When people think they may have injured their shoulder, they often assume the rotator cuff may be the culprit. Most folks over age 50 know someone who has had rotator cuff repair surgery, as it is a relatively common procedure in the United States. A lesser-known source of shoulder pain is that which comes from an inflamed or torn long head biceps tendon.
The biceps muscle of the arm acts to facilitate two main functions in the upper extremity. One is to flex the elbow or help with bringing the hand to the face, and yet despite the fact that many workouts are designed to enhance the size and strength of this muscle, the biceps muscle is in fact not the main power generator in terms of elbow flexion. It is however the most superficial muscle in the front of the arm, so increasing its size through resistance-based exercises certainly has a perceived cosmetic benefit.
Deeper in the arm below the biceps is another larger muscle known as the brachialis. It is the brachialis that is tasked with providing the majority of force aiding elbow flexion. What the biceps brachii is largely responsible for, however, is the power we can muster when turning our palm up, a rotational movement of the forearm known as supination. But as can be inferred from how elbow flexion works, there is redundancy with what powers forearm supination as there is an additional muscle based solely in the forearm that contributes to supination called—you guessed it—the supinator muscle.
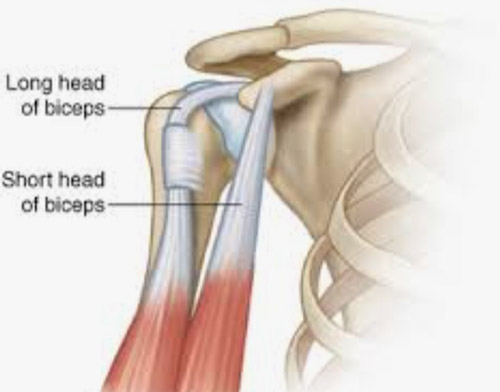
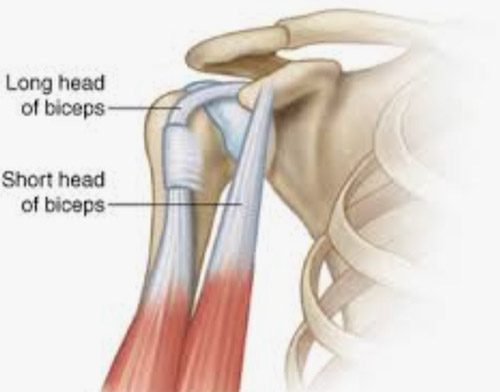
What makes the biceps interesting is that although it inserts as one single tendon in the forearm to power both elbow flexion and forearm supination, it originates above the shoulder joint as two different tendons arising from different locations, hence the bi in biceps!
One of the originating tendons, known as the short head, comes off of a bony process arising from the shoulder blade called the coracoid process. You can feel your own coracoid process by finding the lower border of your collar bone slightly more than midway from the breastbone to the shoulder joint, and if you roll your finger tip down about a finger’s breadth, you’ll feel a tender, hard area under the skin. This is the coracoid process, and the short head of the biceps starts here to then descend down the arm.
The long head of the biceps is even more interesting in that it is one of only two tendons in the body to pass through a joint, that joint being the shoulder. It originates at the top of the socket of the shoulder, which is also part of the shoulder blade, and makes its way through the joint before exiting through an opening in the shoulder capsule, and then travels down the front of the arm to join the short head, completing the biceps muscle. The long head origin of the biceps is called the long head because the total length of the tendon is quite long at 10 cm. This tendon origin doesn’t make the transition to bulkier muscle tissue until almost halfway down the arm.
Like the rotator cuff tendons, the blood supply to the biceps long head becomes tenuous with age. This, combined with the fact that the long head is quite long, means there’s more potential for pathology and disease within this tendon compared to the short head. That’s why when you hear that someone has an issue with their biceps near the shoulder, the long head is almost certainly the culprit. The biceps also is a muscle that crosses two joints, in this case the shoulder and elbow, and any muscle that crosses two joints is often more likely injured due to sometimes poorly coordinated rapid movements where the tendon subsequently experiences extreme tensile forces. The biceps femoris, an analogous hamstring muscle of the thigh which flexes the knee, suffers similar strains for the same reason crossing both the hip and knee.
Like rotator cuff pathology, disease and injury to the biceps long head can be diagnosed by listening to where the patient feels the pain. Often, the pain will be felt radiating down the front of the arm. Sometimes if the long head is torn the patient will experience cramping and fatigue in the arm with repetitive elbow flexion and forearm supination activities. Additionally, the patient may notice the biceps muscle looking balled up in the lower part of the arm. This is known as a Popeye deformity, funnily enough.
MRI is further most helpful in identifying where along the tendon the problem lies. Sometimes the tear can be at the attachment point of the long head to the top of the shoulder socket involving the labral tissue here as well. Other times there can be tearing and inflammation within the long tendinous portion both within the part that travels through the shoulder joint as well as that portion that descends down the front of the arm as the tendon has to make a sharp turn as it leaves the shoulder, only to then travel tightly through a narrow bony groove at the top of the arm. It’s therefore important to identify where the problem lies as this will dictate how the surgeon can best treat it if surgery is needed.
A wide variety of approaches to treating long head biceps pathology has been described in large part due to the various places along the tendon that a problem can arise. And as you can imagine, whenever there’s a lot of solutions to a problem, that often means none of them is very good.
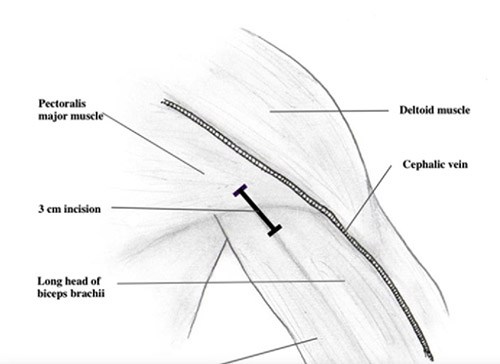
But I would argue that one procedure I often perform to address biceps long head pathology does work well. If surgery is needed, I recommend what’s called the subpectoralis tenodesis. This basically means arthroscopically releasing the long head from its origin at the top of the shoulder socket and then, through a small, cosmetically advantageous incision in the armpit, reattaching the long head to the arm bone below where the pec muscle crosses over. When reattaching the biceps here at this point along its course, you’re affixing the portion of the tendon right before it transitions to muscle, and in doing so, you’re bypassing and essentially removing from the equation most of the 10 cm of tendon that may be inflamed, diseased, or torn. In my 10 years of practice, I’ve had reliably excellent outcomes addressing it this way.
The shoulder is an amazing organ with many moving parts, not the least of which is the long head biceps tendon. Unfortunately, over time, it can succumb to aberrant mechanical forces and the same age-related changes to its tendon biology that typify musculoskeletal disease processes elsewhere in the body. Luckily there is a reliable solution that I’m proud to offer in the form of subpec tenodesis at the Center for Musculoskeletal Disorders.
By Jonathan Lewin, M.D., CMD Health
�





